The baby is finally asleep. The apartment is quiet. Outside, someone is talking in the piazza, a scooter passes, and the light on the buildings looks exactly like the life you imagined when you moved to Italy. Inside, though, you may feel flat, panicked, tearful, angry, or strangely absent from your own life.
If you're an American mother in Italy and you keep wondering why you don't feel grateful, connected, or like yourself, you're not failing at motherhood. You may be dealing with postpartum depression. For many women abroad, the distress is sharpened by distance from family, sleep deprivation, cultural disorientation, and the exhausting task of navigating care in a language that isn't your own. Even practical relocation stress can pile on, which is why broader support around settling abroad, including cultural adaptation and visa tips, can matter more than people realise.
What is postpartum depression? It is a serious, treatable mental health condition after childbirth that goes beyond ordinary adjustment, causing persistent sadness, anxiety, exhaustion, and difficulty functioning. It can make bonding harder, daily tasks feel impossible, and even a beautiful environment feel emotionally unreachable.
I'm Dr. Francesca Adriana Boccalari, Clinical Director at Therapsy. I work with expats and international women in Italy, and I see how often the fantasy of la dolce vita collides with reality of early motherhood abroad. If Mother's Day or family-centred celebrations have felt especially painful, you may also recognise yourself in this reflection on motherhood and emotional complexity.

An Introduction for the American Mom in Italy
Some women describe it this way. “I wanted this baby. I wanted this move. So why do I feel like I'm disappearing?”
That question matters. So does the context around it.
When Italy looks beautiful and life feels unbearable
Living in Italy can create a painful mismatch between appearance and reality. Friends back home may see photos of cobblestone streets, a stylish pram, and a new baby in Milan or Rome. They may assume you're living a dream.
Meanwhile, your actual days may include:
- Isolation at home while your partner works and your support network is on another continent
- Language fatigue when every appointment, pharmacy visit, or form feels harder than it should
- Loss of your old identity because career, friendships, confidence, and independence suddenly feel far away
- Constant self-doubt about whether this is normal new-mother stress or something more serious
Postpartum depression often hides behind ordinary-looking days. A woman can be feeding the baby, answering messages, and still be suffering intensely.
For American women in Italy, one of the hardest parts is the silence around this experience. You may not know which symptoms deserve urgent attention, which professionals to contact, or how to explain what's happening without minimising it yourself.
What Postpartum Depression Is and What It Is Not
Postpartum depression is a severe mental health condition affecting approximately 10 to 20% of women globally following childbirth, with a pooled global prevalence of 17.22%, and it is distinct from the temporary baby blues according to this peer-reviewed review in the National Library of Medicine.
That definition matters because many women dismiss postpartum depression as “just hormones” or “just being overwhelmed”. It isn't.
Postpartum depression is a depressive condition after childbirth that persists, interferes with daily life, and usually needs professional support. It can involve sadness, anxiety, irritability, fatigue, guilt, numbness, hopelessness, and difficulty functioning. Untreated, it can last 3 to 6 months or longer according to the same National Library of Medicine review.
A clear distinction that helps with self-triage
The problem is not that every difficult emotion after birth is postpartum depression. The problem is that women are often told to wait too long before taking their suffering seriously.
Baby blues
Baby blues are common, short-lived emotional changes after birth. You might cry more easily, feel weepy, sensitive, or overwhelmed, but the intensity tends to ease on its own.
In the verified clinical material for this article, baby blues are described as resolving within a short period and not requiring the same level of intervention as postpartum depression.
Postpartum depression
Postpartum depression lasts longer and hits deeper. It doesn't just make you emotional. It can alter how you think, sleep, relate, concentrate, and cope.
It also doesn't always look dramatic. Some women cry constantly. Others feel emotionally blunted and say, “I'm doing everything I'm supposed to do, but I feel nothing.”
Postpartum psychosis
Postpartum psychosis is different from both. It is rare, severe, and requires immediate medical attention. If someone is confused, severely agitated, detached from reality, hearing or seeing things others do not, or is at risk of harming herself or the baby, this is an emergency.
If you feel at risk of harming yourself or your baby, seek urgent emergency support immediately.
Baby blues versus postpartum depression versus postpartum psychosis
| Characteristic | Baby Blues | Postpartum Depression (PPD) | Postpartum Psychosis |
|---|---|---|---|
| Typical intensity | Mild to moderate emotional ups and downs | Significant distress that impairs daily life | Severe psychiatric emergency |
| Duration | Brief and self-limiting | Persists beyond two weeks and may last months if untreated | Acute and urgent |
| Mood pattern | Tearful, sensitive, overwhelmed | Sad, anxious, numb, guilty, hopeless, irritable | Disorganised, confused, detached from reality |
| Functioning | Usually preserved | Often reduced | Severely impaired |
| Need for treatment | Usually monitoring and support | Professional assessment and treatment are often needed | Immediate medical intervention is needed |
If you're also trying to understand whether your symptoms fit a broader depressive picture, this guide on depression and how it presents may help you put words to what you're feeling.
Common Symptoms and Hidden Signs of PPD
Many women expect postpartum depression to feel like obvious sadness. Sometimes it does. Sometimes it feels more like dread, emotional deadness, rage, or a constant sense that you're failing.
Emotional symptoms you may notice first
These are often the symptoms that make a woman think, “Something is wrong, but I don't want to say it out loud.”
- Persistent sadness that doesn't lift, even when things are objectively going well
- Anxiety that feels relentless, especially about the baby, your body, or whether you're coping badly
- Irritability or anger that feels out of proportion to the situation
- Guilt and shame about not enjoying motherhood the way you expected
- Hopelessness or the sense that this version of life will never improve
- Emotional numbness rather than visible distress
Behavioural and cognitive signs that families often miss
Sometimes the strongest clue is not what you feel, but what becomes harder to do.
- You withdraw. You stop replying to friends, avoid calls home, or cancel plans because interacting feels exhausting.
- You lose interest. Things that normally comfort you, including food, music, exercise, or walking through your neighbourhood, no longer reach you.
- Your concentration drops. You forget simple tasks, can't make decisions, or feel mentally foggy all day.
- Sleep becomes complicated. You may struggle to sleep even when the baby sleeps, or want to sleep all the time but never feel restored.
- Bonding feels harder than expected. This can look like distance, fear, guilt, or panic rather than lack of love.
A mother can love her baby deeply and still feel disconnected, frightened, or depressed. Those experiences do not cancel each other out.
Physical symptoms that get mistaken for ordinary exhaustion
In Italy, psychological distress is often expressed physically, and new mothers often dismiss these signs because postpartum life is tiring by definition.
Look out for:
- Chronic fatigue that feels heavier than sleep deprivation alone
- Appetite changes in either direction
- Restlessness that keeps your body tense even when you sit down
- Somatic complaints such as headaches, stomach discomfort, or a persistent sense of being physically unwell
What high-functioning PPD can look like
This matters a great deal for American women who are used to being competent, productive, and self-managing.
High-functioning postpartum depression can look like:
- You keep the baby appointments and answer emails, but cry in the shower or feel dread every evening
- You appear organised, yet internally feel detached, frightened, or trapped
- You tell everyone you're “just tired”, while your mind keeps cycling through guilt and self-criticism
- You compare yourself harshly to mothers online, to Italian mothers around you, or to the version of yourself you thought you'd be
If that sounds familiar, you may recognise similar patterns in this guide to high-functioning depression signs.
Why Does PPD Happen Causes and Risk Factors
Postpartum depression does not come from weakness, poor gratitude, or a bad attitude. It develops through a mix of biological vulnerability, psychological stress, and social context.
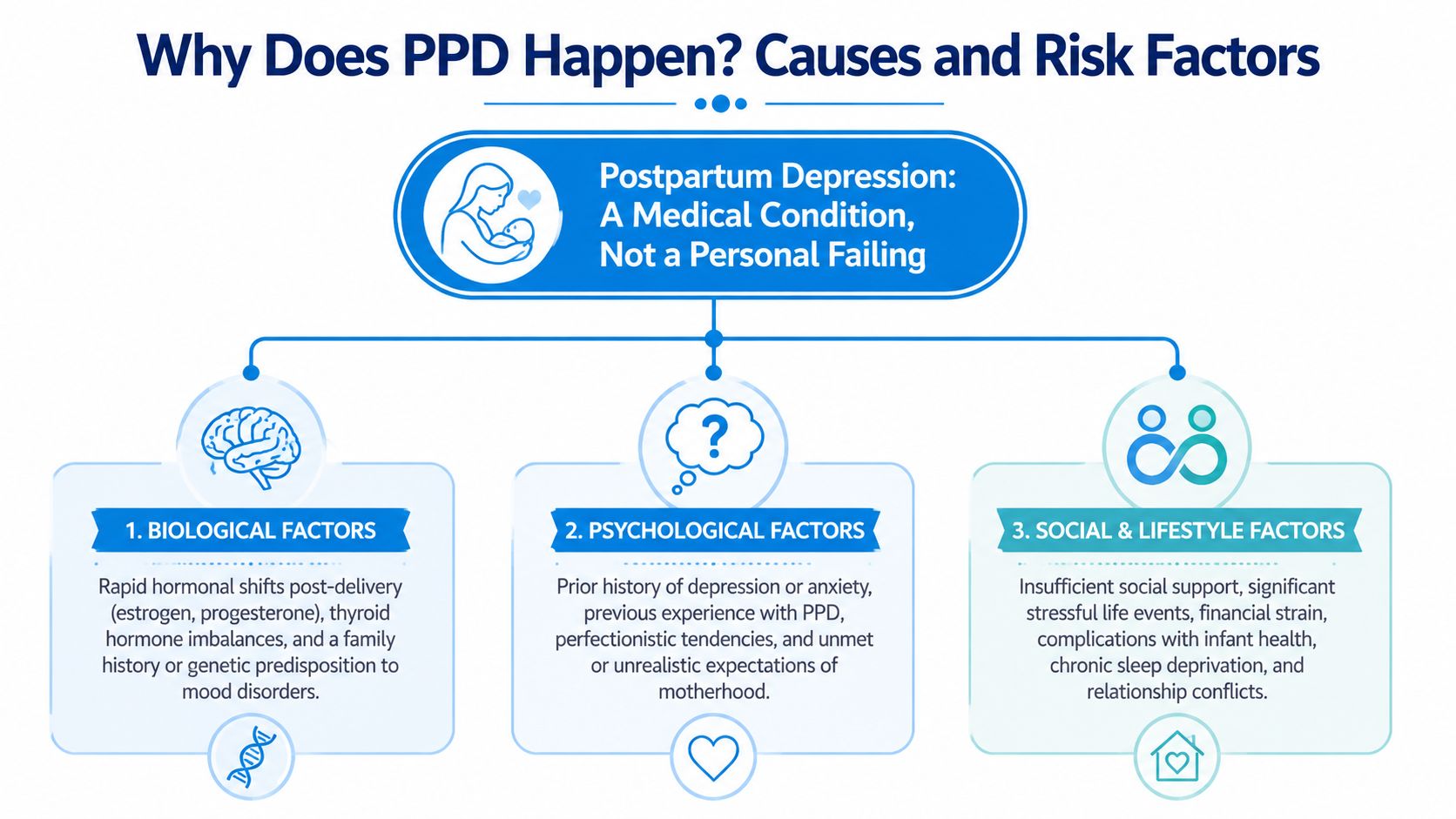
The biopsychosocial picture
A useful clinical framework is the biopsychosocial model. It helps explain why two women can have similar births but very different emotional outcomes.
Biological factors
Postpartum depression has real neurobiological underpinnings. Verified clinical material describes converging biological pathways involving neurotrophic changes, cerebral hypoperfusion, nitric oxide-mediated neurotoxicity, hyperprolactinemia-related receptor changes, and reward system impairment.
For a readable explanation of how the brain can change during this period, some women find understanding PPD brain changes useful alongside formal clinical care.
A history of depression also matters because vulnerability can return under perinatal stress. Verified data indicates that PPD has a recurrence risk of 25 to 40% in subsequent deliveries, with approximately 24% of recurrences appearing within the first two weeks postpartum according to the Italian National Institute of Health information cited here.
Psychological factors
Cognitive Behavioural Therapy, or CBT, helps us understand how thoughts, emotions, body states, and behaviour reinforce one another. A mother who is exhausted and isolated may begin thinking, “I'm a bad mother”, then feel more despair, withdraw more, and lose corrective support.
Schema Therapy adds another layer. Women with strong perfectionism, self-sacrifice, or unrelenting standards often suffer intensely because motherhood activates old beliefs such as “I must cope alone” or “needing help means I'm failing.”
Social factors
The social environment can either buffer stress or magnify it. Lack of sleep, conflict with a partner, financial strain, feeding difficulties, and loss of routine can all increase vulnerability.
Attachment theory also matters here. When a mother feels unsupported, unsafe, or emotionally alone, her nervous system stays activated. Recovery becomes harder because her body never gets the message that help is present.
Postpartum depression is a medical and psychological condition. It is not a verdict on your love for your child.
Expat-specific risk factors for American women in Italy
The Italy story changes the picture at this point.
Verified data for this article notes that immigrant women in Italy face a 3x higher risk of perinatal depression due to social isolation and limited access to culturally competent care according to the Italian National Institute of Health.
For American women, the gap between expectation and reality can be brutal:
- The missing village. Your mother, sister, best friend, or trusted postpartum support may be in another country.
- The romanticised Italy dream. You may feel ashamed that you're unhappy in a place others envy.
- Language barriers in care. Explaining fear, intrusive thoughts, or numbness in another language can feel impossible.
- Identity loss. Work, autonomy, and your familiar social self may vanish overnight.
- Bureaucratic stress. Forms, appointments, referrals, and healthcare navigation consume energy you don't have.
Cross-cultural psychology teaches that distress often rises when external change is rapid and internal support is thin. Motherhood abroad is exactly that combination.
Getting Help in Italy Screening and Diagnosis
Many women delay care because they think they need to be completely sure before speaking to someone. You don't. You only need enough concern to ask for an assessment.
What screening usually looks like
In Italy, the Ministry of Health recommends universal postpartum depression screening with the Edinburgh Postnatal Depression Scale (EPDS) at 1, 3, and 6 months postpartum, according to the Italian Ministry of Health. The same verified data also states that up to 50% of women with PPD never receive a formal diagnosis, which is one reason early conversation matters.
The EPDS is a screening tool, not a final diagnosis. It helps identify whether your symptoms deserve closer clinical attention.
A proper assessment usually includes:
- Your symptom pattern, including mood, anxiety, sleep, appetite, functioning, and thoughts
- Timing, especially when symptoms started and whether they are worsening
- Context, such as birth experience, relationship stress, prior mental health history, and available support
- Safety, including any thoughts of self-harm or fear of harming the baby
Who to contact in Italy
The Italian system can feel confusing when you're already overwhelmed.
Your medico di base
Your medico di base is your general practitioner. This can be a useful first contact, especially if you need referrals, medical screening, or documentation. The downside for many expats is communication difficulty and variable familiarity with perinatal mental health.
A psychologist
A psychologist or psychotherapist assesses emotional symptoms and provides psychotherapy. If your main need is to understand what's happening and begin treatment, this is often the most direct route.
A psychiatrist
A psychiatrist evaluates whether medication may help, especially when symptoms are more severe, persistent, or complicated by sleep collapse, high anxiety, or safety concerns.
If you're unsure which professional fits your situation, this guide on psychologist versus psychiatrist in Italy can make the decision clearer.
Public and private routes in practice
The SSN, or Italian National Health Service, can provide access to psychotherapy and psychiatric consultation for postpartum depression. In reality, wait times and language access can make the process difficult, especially when symptoms need timely attention.
The private route is often faster and simpler for expats, but women understandably worry about choosing the right clinician, being understood culturally, and not having to retell everything to multiple people.
The best first step is not choosing the perfect treatment. It is getting accurately understood.
What to say if you don't know how to start
You don't need polished language. A simple script is enough:
- Say what is changing. “Since the birth, I feel persistently low, anxious, and unlike myself.”
- Name the impact. “It's affecting my sleep, my concentration, and my ability to function.”
- Mention the duration. “It's not passing.”
- State urgency. “I need an assessment in English.”
If speaking in Italian feels impossible, write your symptoms down in English first. Bring notes. Ask directly whether the professional has experience with postpartum mental health and with international patients.
Evidence-Based Treatments for Postpartum Depression
Postpartum depression is treatable. The most effective treatment depends on severity, risk factors, practical circumstances, and what you can realistically access and sustain.
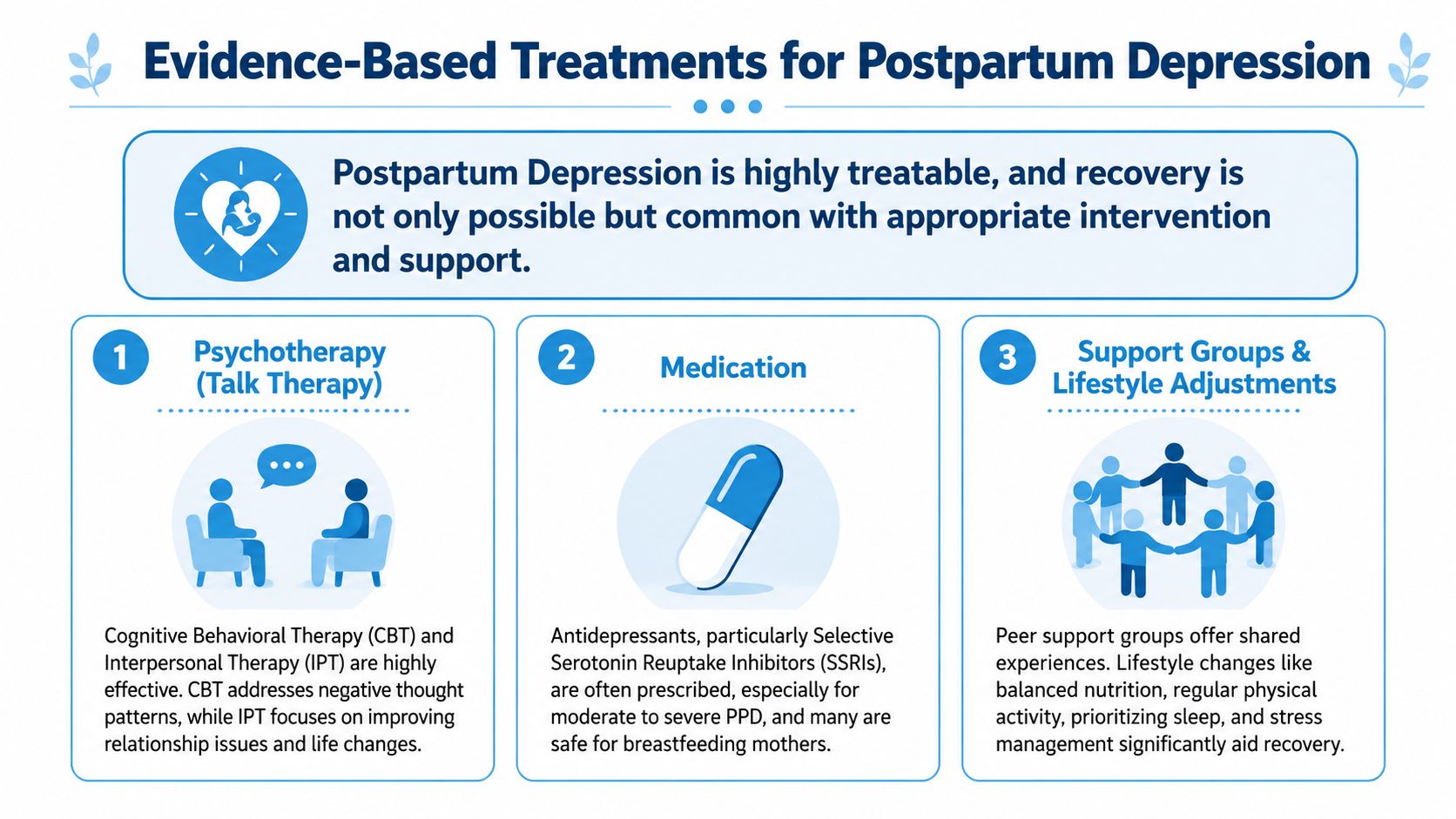
Psychotherapy often forms the core of care
For many mothers, therapy is the place where the chaos finally becomes coherent.
CBT
Cognitive Behavioural Therapy helps identify the thought loops and behavioural patterns that keep depression going. In postpartum work, that often includes perfectionism, catastrophic thinking, guilt, avoidance, and the belief that asking for help is weakness.
CBT works well because it is practical. It helps you test thoughts, regulate routines, reduce self-attack, and build coping strategies that fit the reality of life with a baby.
If you want a straightforward overview, this introduction to Cognitive Behavioural Therapy explains how the method works.
IPT
Interpersonal Therapy is strongly relevant in the postpartum period because so much distress is tied to role transition, conflict, loneliness, grief, and changed relationships. For expats, that can include separation from family and disappointment in a partner who may also be struggling.
EMDR
EMDR can be useful when postpartum depression is entwined with trauma. That may include a frightening birth, emergency intervention, NICU stress, or older unresolved experiences that become activated after childbirth.
EMDR does not erase memory. It helps the brain process distressing experiences so they stop overwhelming the present.
Medication can be appropriate and helpful
Medication is not a failure of coping. For moderate to severe postpartum depression, it can be an important part of recovery.
Verified clinical data for this article notes that treatment can include SSRIs such as sertraline, and that sertraline is approved for breastfeeding within the clinical material provided. Medication decisions should always be made with a qualified prescriber who can assess your symptoms, medical history, breastfeeding considerations, and preferences.
Medication tends to work best when:
- Symptoms are intense and daily functioning is significantly impaired
- Anxiety is constant and your nervous system feels unable to settle
- Sleep has collapsed beyond what infant care alone would explain
- Therapy alone isn't enough or doesn't feel accessible quickly enough
What usually does not work well on its own
There are supportive habits that matter, but they are not substitutes for treatment when depression is established.
What often falls short on its own:
- Trying harder
- Waiting for gratitude to appear
- Telling yourself this is just what motherhood is
- Scrolling for reassurance while getting more overwhelmed
- Relying only on a few hours of sleep or one good day as proof you're fine
Recovery usually begins when support becomes structured, regular, and specific.
Building Your Support System and Self-Help Strategies
Professional treatment matters, but daily support also matters. The aim is not to create a perfect routine. It is to reduce overload and increase steadiness.
Small self-help steps that genuinely help
Choose what is realistic, not what sounds impressive.
- Lower the standard for the day. A day can count as successful if you and the baby are safe, fed, and cared for.
- Use body-based regulation. Eat regularly, drink water, step outside, and notice whether your nervous system softens even slightly after movement or fresh air.
- Accept practical help in concrete form. Ask for one meal, one errand, one baby-holding shift, or one appointment call.
- Reduce secrecy. Tell one trusted person the truth in one sentence. “I'm not doing well and I need support.”
What partners and family can do better
“Tell me what you need” is kind, but it often asks too much of a depleted mother.
More helpful support sounds like this:
- Make offers specific. “I'll take the baby for the next hour.” “I'll handle dinner.” “I'll come with you to the appointment.”
- Listen without correcting. Don't rush to say she's doing great if she's trying to tell you she feels terrible.
- Watch functioning, not appearances. A mother can look composed and still be in real danger emotionally.
- Take talk of hopelessness seriously. If she mentions feeling unsafe, unable to cope, or afraid of her own thoughts, act immediately.
For expat families, support may also need to be international. Ask relatives abroad for targeted help such as booking a flight, arranging meal delivery, funding temporary assistance, or staying on video call during difficult hours.
FAQ
Is postpartum depression common after having a baby in Italy
Yes, postpartum depression is common enough that it should never be dismissed as unusual. Verified data for this article notes that postpartum depression affects a substantial share of women globally and that Italy also sees significant rates, particularly among women facing stress, isolation, or barriers to care.
How do I know if it is baby blues or postpartum depression
The simplest rule is duration and impact. If your symptoms persist beyond the early brief adjustment period, feel intense, or interfere with sleep, bonding, functioning, or safety, it's time to seek a professional assessment.
Can I have postpartum depression even if I love my baby
Yes, absolutely. Love for your baby and depression can exist at the same time, and many mothers feel intense guilt because they assume they cannot.
What if I don't speak Italian well enough to ask for help
You can still get help, and language barriers should not stop you from seeking it. Write your symptoms in English, bring notes to appointments, and look for an English-speaking psychologist, psychotherapist, or psychiatrist who understands expat life in Italy.
Is postpartum depression treatable
Yes, postpartum depression is treatable. Evidence-based care often includes psychotherapy, and sometimes medication, with treatment adapted to severity, history, and what feels safe and practical for the mother.
When should I seek urgent help
Seek urgent help immediately if you feel you may harm yourself or your baby, if you feel detached from reality, or if your thoughts become frightening and unmanageable. Those signs need rapid medical attention, not watchful waiting.
Book your first free assessment call. There's no commitment, just a conversation with our Clinical Director who will listen and match you with the right therapist for you. Visit Therapsy.
Dr. Francesca Adriana Boccalari, Clinical Director at Therapsy










